Lyrica (pregabalin), when used on its own for fibromyalgia, is superior to opioids in reducing pain and improving pain interference in daily life, finds a study sponsored by Pfizer.
The analysis, which included 1,421 fibromyalgia patients, showed that those using Lyrica doses recommended for fibromyalgia treatment had the best outcomes, suggesting that many patients should increase their doses to reach recommended levels.
Pfizer and ProCare Systems conducted the study, “Interpreting the Effectiveness of Opioids and Pregabalin for Pain Severity, Pain Interference, and Fatigue in Fibromyalgia Patients,” which took aim at the notion that — despite little evidence of their effectivity — opioids are the most commonly prescribed drugs for fibromyalgia. To examine how different treatments affect pain and related outcomes in fibromyalgia patients, the research team turned to information from the ProCare Systems network of chronic pain clinics in Michigan.
All patients received Lyrica or opioids alone or in combination, and had been through several pain health assessments, including pain characteristics, physical function, and psychosocial function.
The team divided the patients into different groups based on their average morphine equivalent dose or average Lyrica dose. Patients were followed between 56 and 365 days. Nearly 78 percent of them were women — typical of fibromyalgia in the real world.
Findings, published in the journal Pain Practice, showed that only 3.4 percent of patients took the recommended Lyrica dose of 300-450 mg. Most patients took less than 150 mg of Lyrica, either alone or combined with high-dose opioids.
The team assessed the number of patients in the different medication groups and noted that more of those who took Lyrica without opioids achieved at least 30 percent improvement across all pain measurements.
Lyrica treatment was also superior to opioids or opioid-Lyrica combinations in improving pain-related aspects, such as “ability to enjoy life, activity in general, mood and sleep.” The only pain-related aspect that was better in the group combining Lyrica and moderate doses of opioids was “relationships with others.”
When increasing the threshold to at least 50 percent improvement in pain and pain-related aspects of daily living, Lyrica was again superior to opioids or combinations.
While Lyrica did score low on how well it affected fatigue, it did better when combined with moderate opioid doses.
“Pregabalin without opioids provided the most favorable outcomes overall based on ≥30% and ≥50% improvement thresholds … with support for moderate … opioids+pregabalin in patients suffering from fatigue” researchers wrote.
Researchers also noted that patients taking higher Lyrica doses, reaching the recommended dose range, had better outcomes than those taking low doses.
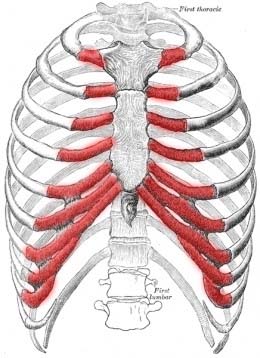
Many fibro patients suffer from a condition called Costochondritis, apart from common symptoms of fibromyalgia. In this condition, wearing a bra becomes difficult and sometimes even becomes impossible because it causes pain in the rib cage and breasts. Wearing the right bra can reduce the pain significantly if you are suffering from Costochondritis.
Inflammation of the cartilage that links the ribs to the breast bone is Costochondritis. It is very sudden and causes immense chest pain, much of fibromyalgia pain begins with this pain. Is the pain mildly irritating or it is extremely irritating, this all depends on the amount of inflammation, patients suffer from. Some patients describe what they go through as burning, stabbing, or aching pain. Some patients suffer from a complex chain of pain that they even relate to a heart attack.
In this condition, it is a painful task to put on tight clothing which compresses the ribs and needless to say an underwear bra. To reduce the pain wearing a comfortable bra is necessary to get rid of breast and ribcage inflammation but many women do not do this. However, when needed, it is best to wear something not too tight, in a comfortable fabric, and easy to wear and remove. Here are some tips for the selection of the right bra:
Seamless bra types are ideal as they prevent edgings from pressing against the skin.
Prevent that type of fiber that brushes against the skin and causes pain by avoiding anything textured like lace, tulle, or fabric with embroidery.
Best bra styles for every size
Soft cup bras: these bras offer good support for women of all sizes. Choose something with wilder shoulder straps as they won’t dig into the skin like the thinner ones do. A front closure design would also reduce the pain of putting on and removing the bra.
Sports bras: these bras can be very easy and comfortable as they give support to women of all sizes. Opt for something softer and with a wider stretch to prevent squeezing your ribcage and causing pain.
Bralettes: for smaller-sized women, a bralette might work in a good way. They are usually made with soft cups and are mildly comfortable.
Bandeaus: it is another good option for small and medium-sized women because bandeaus will sure that no wires or edges would press against the skin.
After two hourlong sessions focused first on body awareness and then on movement retraining at the Feldenkrais Institute of New York, I understood what it meant to experience an incredible lightness of being. Having, temporarily at least, released the muscle tension that aggravates my back and hip pain, I felt like I was walking on air.
I had long refrained from writing about this method of countering pain because I thought it was some sort of New Age gobbledygook with no scientific basis. Boy, was I wrong!
The Feldenkrais method is one of several increasingly popular movement techniques, similar to the Alexander technique, that attempt to better integrate the connections between mind and body. By becoming aware of how one’s body interacts with its surroundings and learning how to behave in less stressful ways, it becomes possible to relinquish habitual movement patterns that cause or contribute to chronic pain.
The method was developed by Moshe Feldenkrais, an Israeli physicist, mechanical engineer, and expert in martial arts after a knee injury threatened to leave him unable to walk. Relying on his expert knowledge of gravity and the mechanics of motion, he developed exercises to help teach the body easier, more efficient ways to move.
I went to the institute at the urging of Cathryn Jakobson Ramin, author of the recently published book “Crooked” which details the nature and results of virtually every current approach to treating back pain, a problem that has plagued me on and off (now mostly on) for decades. Having benefited from Feldenkrais lessons herself, Ms. Ramin had good reason to believe they would help me.
In her book, she recounts the experience of Courtney King, who first experienced crippling back spasms in her late 20s. Ms. King was taking several dance classes a week and practicing yoga, and she thought the stress of these activities might be causing the pain in her tight, inflexible back. But after a number of Feldenkrais sessions, she told Ms. Ramin, “I realized that the pain had more to do with the way I carried myself every day.”
Even after just one session, I understood what she meant. When I make a point of walking upright and fluid, sitting straight, even cooking relaxed and unhurried, I have no pain. The slow, gentle, repetitive movements I practiced in a Feldenkrais group class helped foster an awareness of how I use my body in relation to my environment, and awareness is the first step to changing one’s behavior.
One common problem of which I’m often guilty is using small muscles to accomplish tasks meant for large, heavy-duty ones, resulting in undue fatigue and pain.
The group class, called Awareness Through Movement, was followed by an individual session called Functional Integration with a therapist that helped to free tight muscles and joints that were limiting my motion and increasing my discomfort. Using gentle manipulation and passive movements, the therapist individualized his approach to my particular needs.
The ultimate goal of both sessions is, in effect, to retrain the brain – to establish new neural pathways that result in easy, simple movements that are physiologically effective and comfortable. Although the Feldenkrais method was developed in the mid-20th century, neurophysiologists have since demonstrated the plasticity of the brain, its ability to form new cells, reorganize itself, and, in effect, learn new ways to do things.
The beauty of Feldenkrais lessons is that they are both relatively low-cost (group classes average $15 to $25, individual sessions $100 to $200) and potentially accessible to nearly everyone. There are more than 7,000 teachers and practitioners working in 18 countries, including large numbers in the United States. You can be any age, strength, fitness level, and state of well-being to participate. The exercises are slow, gentle, and adjustable to whatever might ail you. Their calming effect counters the stress that results in contracted muscles, tightness, and pain.
Many Feldenkrais practitioners, like Marek Wyszynski, director of the New York center, start professional life as physical therapists, although many other practitioners begin with no medical background. They then undergo three and a half years of training to become certified in the Feldenkrais Method.
Mr. Wyszynski explained that he starts by observing how patients are using their skeletons – how they sit, stand, and walk-in ways that may cause or contribute to their pathology, be it spinal disc disease, arthritis, shoulder pain, or damaged knee joints. In accordance with Dr. Feldenkrais’s astute observation, “If you don’t know what you are doing, you can’t do what you want,” patients are then given a clear sensory experience of how their posture and behavior contribute to their pain and physical limitations.
For example, some people may use excessive force, clench their teeth, hold their breath, or rush, causing undue muscle tension and skeletal stress. Years ago, I realized that my frequent headaches resulted from an unconscious habit of clenching my jaw when I concentrated intently on a task like sewing or cooking. Feldenkrais teachers do not give formulas for a proper way of behaving; rather, they rely on their patients’ ability to self-discover and self-correct.
Once aware of their counterproductive habits, students are given the opportunity to experience alternative movements, postures, and behaviors and, through practice, create new habits that are less likely to cause pain.
Mr. Wyszynski told me that there are more than 1,000 distinct Feldenkrais lessons currently available, most of which involve everyday actions like reaching, getting up from a chair, turning, bending, and walking.
As a mechanical engineer and physicist, Dr. Feldenkrais understood that the job of the human skeleton was to accommodate the effects of gravity in order to remain upright. And he wanted people to achieve this in the most efficient way possible.
Using two tall foam cylinders, one perched on top of the other, Mr. Wyszynski demonstrated a guiding principle of the Feldenkrais Method. When the top cylinder was centered on the bottom one, it stood in place without assistance. But when it was off-center, perched near the edge of the bottom cylinder, it tipped over. If instead of cylinders these were someone’s skeletal parts that were askew, tightened muscles would have to keep the patient from falling over.
As Mr. Wyszynski explained, “Good posture allows the skeleton to hold up and support the body without expending unnecessary energy despite the pull of gravity. However, with poor posture, the muscles are doing part of the job of the bones, and with poor skeletal support, the muscles have to remain contracted to prevent the body from falling.”
Throughout the history of Fibromyalgia, this disease has been strangely hard to identify and analyze on the grounds that it shows up, at first look, to be something else. Perhaps its symptoms including musculoskeletal pain, fatigue, mood swings, and memory loss, are genuinely common. To give some point of view 1 in 70 people, almost ladies, in the US really have fibromyalgia.
However, there is stunning news for all of us. For those who have this horrible condition, hyperbaric oxygen treatment has made some diversion changing ground in medicine. Women who attempted hyperbaric oxygen treatments were able to reduce or completely wipe out their requirements for pain medication, found by the Researchers from Tel Aviv University.
As per beliefs of Researchers, the primary cause of fibromyalgia is a disturbance of brain mechanisms that are responsible for processing pain.
“For me, as a physician, the most important finding is that 70 percent of the patients could recuperate from their fibromyalgia symptoms. For the world of research, the most amazing finding, however, is that we were able to map the malfunctioning brain regions responsible for the syndrome… The intake of [the pain medication they were taking] facilitated the pain but did not reverse the condition. But hyperbaric oxygen treatments actually reverse the condition…
Hyperbaric oxygen treatments are designed to address the actual reason for fibromyalgia – the brain pathology in charge of the syndrome.
Dysphagia is a medical term that means that a patient has difficulty swallowing. There are a number of different conditions that can cause dysphagia. And someone who suffers from dysphagia often finds that it makes life very difficult. Depending on their condition, swallowing can be very painful, which makes eating and getting enough nutrition a challenge.
And what’s even more alarming is that many people with fibromyalgia report having problems with dysphagia.
So, what are some of the things that can cause dysphagia? Is there a link between the condition and fibromyalgia? And what can you do to treat it?
There are a number of different things that can cause dysphagia. Anything that interferes with the complex system of nerves and muscles that control the esophagus can make swallowing difficult. But some of the most common causes are:
Achalasia– a condition that causes the muscles in the esophagus to constrict.
Diffuse Spasm– a condition where the muscles spasm uncontrollably, usually after swallowing.
Esophageal Stricture– a narrowing of the opening of the esophagus caused by scar tissue or tumors.
Gastro-Intestinal Reflux Disease (GERD)– The gradual destruction of the tissue in the esophagus caused by acid from the stomach washing up into the esophagus.
Dysphagia can also occur without any obvious source. But whatever the cause, the symptoms are often similar. The most common symptoms are difficulty swallowing, pain in the throat, frequent heartburn, a hoarse voice, and regurgitating food you’ve already eaten.
In most cases, dysphagia isn’t dangerous. But it can lead to dramatic weight loss and can be life-threatening if it causes you to regurgitate food into the lungs.
And while we don’t always know what causes the condition, we do know that it is abnormally common in people with fibromyalgia.
A study by the National Institute of Health in the United States determined that a significant number of patients with fibromyalgia reported problems with swallowing. Patients in the study reported suffering from dysphagia at a rate 40% higher than people without fibromyalgia.
Unfortunately, the reason this sort of symptom is common in people with fibromyalgia remains a mystery. There’s so much that we don’t know about how fibromyalgia works, including why it would cause dysphagia. But we can speculate on a number of possibilities.
People with fibromyalgia often experience muscle weakness. This weakness could explain why they suffer from dysphagia. The muscles that control the process of swallowing may be affected by the general weakness caused by fibromyalgia.
In addition, we know that people with fibromyalgia have problems with their nervous system. An NIH study found that patients with fibro had significantly more neurological abnormalities than a control group. If fibromyalgia is a condition that affects the nervous system, as many doctors suggest it is, then it could be causing a breakdown between the nerves that control the esophagus and the brain.
This would explain why people with fibromyalgia have a hard time swallowing. Their brain can’t control the muscles in the esophagus as they normally would. But until we know more about the condition, we can’t say for sure what the link is. Luckily, there are some things you can do to treat the condition.
The first step in treatment is a diagnosis. The most common way to diagnose the condition is with an imaging test, like a barium X-ray. Essentially, the patient drinks a contrast material – barium- which coats the esophagus and makes it easier to see on the X-ray. The doctor can then examine the image to see if your esophagus is expanding correctly. And this examination can also be done with an endoscopic camera.
Your treatment will depend on what’s causing the condition. If the condition is caused by weakened muscles, there are a number of exercises you can do to strengthen the muscles. And you can learn different swallowing techniques to compensate for the weakened muscles. Your doctor will be able to advise you on what to do.
If the treatment is caused by muscle constriction in the esophagus, there are a number of medications that can help relax the muscles. In addition, a surgeon can perform a procedure to dilate the muscles and force them to relax. Finally, a surgeon can remove portions of the esophagus to widen the space for food to pass through.
If you’re experiencing difficulties swallowing, it’s always a good idea to see a doctor. They will be able to give you advice on the best course of treatment.
Thyme is an herb from the mint family. This is a truly ancient herb, used by the Egyptians, Greeks, and Romans for ceremonial and ritualistic purposes. Through the Middle Ages where it was also used for religious and medicinal reasons. It is an incredibly potent yet simple herb affecting multiple systems in the body and capable of treating dozens of diseases. It contains one of the strongest antioxidants known and is proven to kill 98% of breast cancer cells.
Thyme contains thymol which is a natural antiseptic, antibacterial, and an expectorant, making this tea with honey and lemon a delicious remedy for all of you suffering from sore throats and coughs.
Wild thyme tea is recommended for cough, hangover, flu, and sore throat. Thyme has primarily been used for respiratory ailments for its infection-fighting and cough suppressive qualities. Thyme honey is ideal for sweetening herb teas. Blend thyme with nettle for allergies and mints for colds and congestion. It is also help’s if you have fibromyalgia, rheumatoid arthritis, lupus & multiple sclerosis.
-1c Boiling Water -1tbs dry or 1T fresh Thyme -1tbs dry or 1T fresh sage -1-1 Ginger slices -Honey to taste
Directions: -Warm your teacup with hot water. -Pour away the water. -Put herbs in the cup. Add fresh boiling water and cover. -Leave to steep 3 to 5 minutes. Add more herbs for a stronger flavor. -Steeping too long will make the tea bitter. Use Honey or a natural herbal sweetener like Stevia. -Add ginger slices and/or lemon slices if desired.
Light and noise sensitivity in fibromyalgia (FMS) and chronic fatigue syndrome (ME/CFS) have been scientifically established since the early 1990s, but they’re still underrecognized and rarely make symptoms lists. Rest assured that you’re not alone in experiencing this symptom!
When I used to take my kids to daycare, some mornings the noise would hit me like a brick wall. In an instant, I’d have pain, nausea, dizziness, trembling, and a looming panic attack.
More than once, I had to call in sick as a result of it. I’ve had similar experiences with bright or flashing lights, or with visual chaos in general.
We don’t know the causes of light and noise sensitivity, but they’re often called “generalized hypervigilance.” That means our bodies are constantly on high alert. It’s also a symptom of post-traumatic stress disorder.
Hypervigilance is beneficial for people in potentially dangerous situations, such as soldiers or police officers, because it speeds up to several processes and helps with crisis response.
In FMS and ME/CFS, however, hypervigilance overwhelms us. We don’t know why, but possibilities include:
So far, we don’t have research showing that specific treatments alleviate light and noise sensitivity in FMS and ME/CFS.
In people with PTSD, treatment for the anxiety related to generalized hypervigilance can include mental-health counseling and medications, especially antidepressants.
Supplements for anxiety and stress may help you cope better with light and noise sensitivity as well. Some people also benefit from treatments such as massage or acupuncture.
Light and noise sensitivity can have a huge impact on your life. You may avoid certain situations and even fear them, which increases anxiety. It can also contribute to social isolation, which is common in people with FMS or ME/CFS and can worsen depression.
Some work environments are difficult to endure. I used to be a television news producer, which meant sitting under a lighting grid in a room with dozens of TVs and ringing phones. I went from thriving in the chaos to having regular anxiety attacks. I decided to leave the job. Other people may be able to get reasonable accommodation to lessen the impact of this symptom.
You might be able to eliminate or avoid many sources of excess noise and light, but you probably can’t eliminate all of them. Several simple things can help you deal with light and noise sensitivity in your daily life:
If fluorescent lights bother you, lightly tinted sunglasses or a hat with a brim may help.
In a noisy environment, earplugs or listening to music on headphones may help some people.
Deep breathing and other relaxation techniques can help you get through episodes of sensory overload due to light and noise.
Teach your family and friends about the impact that light and noise have on you so they understand your requests to turn off lights or turn down the volume.
If your computer screen bothers you, try adjusting the brightness and contrast.
Many fibromyalgia sufferers have been told that the pain is “all in their head.” New research indicates there may be some truth to that, and that overactive brain networks could play a role in the hypersensitivity of fibromyalgia patients.
Fibromyalgia is a poorly understood disorder characterized by deep tissue pain, fatigue, headaches, mood swings, and insomnia. There is no known cause and successful treatments have been elusive.
In a lengthy study published in the journal Scientific Reports, an international team of researchers at the University of Michigan and in South Korea report that patients with fibromyalgia have brain networks primed for rapid responses to minor changes. This abnormal hypersensitivity is known as called explosive synchronization (ES).
“For the first time, this research shows that the hypersensitivity experienced by chronic pain patients may result from hypersensitive brain networks,” says co-senior author Richard Harris, Ph.D., an associate professor of anesthesiology at Michigan Medicine’s Chronic Pain and Fatigue Research Center.
In ES, a small stimulus can lead to a dramatic synchronized reaction throughout the network, as can happen when a power outage triggers a major grid failure or blackout. Until recently, this phenomenon was studied in physics rather than medicine. Researchers say it’s a promising avenue to explore in the quest to determine how a person develops fibromyalgia.
“As opposed to the normal process of gradually linking up different centers in the brain after a stimulus, chronic pain patients have conditions that predispose them to link up in an abrupt, explosive manner,” says first author UnCheol Lee, PhD., a physicist and assistant professor of anesthesiology at Michigan Medicine.
The researchers tested their theory by conducting electroencephalogram (EEG) tests on the brains of 10 female patients with fibromyalgia. Baseline EEG results showed the patients had hypersensitive brain networks, and that there was a strong correlation between the degree of ES conditions and the self-reported intensity of their pain during EEG testing.
Lee’s research team and collaborators in South Korea then used computer models of brain activity to compare the stimulus responses of the fibromyalgia patients to those of healthy ones. As expected, the fibromyalgia model was more sensitive to electrical stimulation.
“We again see the chronic pain brain is electrically unstable and sensitive,” Harris says.
Harris says this type of modeling could help guide future treatments for fibromyalgia. Since ES can be modeled outside of the brain in computers, researchers can test for influential regions that transform a hypersensitive network into a more stable one. These regions could then be targeted in living humans using noninvasive brain modulation therapies such as transcranial magnetic stimulation, which is currently used to treat fibromyalgia and depression.
“We expect that our study may ultimately suggest new approaches for analgesic treatments. ES provides a theoretical framework and quantitative approach to test interventions that shift a hypersensitive brain network to a more normal brain network,” researchers reported.
“It may be possible to convert an ES network to a non-ES network just by modulating one or two hub nodes. Indeed, transcranial magnetic stimulation and/or transcranial direct current stimulation may be improved by ‘targeting’ these sensitive hub nodes. The application of deep brain stimulation to critical nodes that could modify ES conditions is another therapeutic possibility that could be explored.”
Let’s be perfectly honest. Most doctors have a difficult time with chronic pain patients. One physician described it to us many years ago: “When I see a patient suffering severe chronic pain come in the front door I want to go out the back door.” That’s because there are few good options. Drugs like hydrocodone or oxycodone used to be prescribed in huge quantities. Now gabapentin (Neurontin) and pregabalin (Lyrica) are on the ascendency and opioids are shunned. The Opioid Epidemic: Doctors are dismayed by the opioid epidemic sweeping the nation. Over the last year, the drumbeat of headlines about opioid overdoses and deaths has scared a lot of physicians into cutting back on prescribing drugs like hydrocodone or oxycodone.
Many of the overdose deaths are caused by illicit fentanyl. People OD because they have no idea how potent the narcotics are that they are snorting, swallowing, or injecting. According to the CDC (Nov. 3, 2017):
“Preliminary estimates of U.S. drug overdose deaths exceeded 60,000 in 2016 and were partially driven by a fivefold increase in overdose deaths involving synthetic opioids (excluding methadone), from 3,105 in 2013 to approximately 20,000 in 2016. Illicitly manufactured fentanyl, a synthetic opioid 50–100 times more potent than morphine, is primarily responsible for this rapid increase. In addition, fentanyl analogs such as acetylfentanyl, furanylfentanyl, and carfentanil are being detected increasingly in overdose deaths and the illicit opioid drug supply.”
Fentanyl powder does not come from your local pharmacy. Most of it is illicit and is coming from foreign countries (CBS News; New York Times, Aug. 10, 2017). China and Mexico are major suppliers. It is being added to heroin or even counterfeit opioid pills that look like Percocet (CNN June 8, 2017) or Oxycontin. The government does not seem to know how to stem the flow of illicit fentanyl that is flooding the country. Doctors and Opioids: It is hardly any wonder that doctors have cut back on prescriptions for hydrocodone and oxycodone. Like the rest of us, they read horrifying reports about opioid deaths. The evening news often leads with graphic accounts of accidental overdoses. Federal guidelines and restrictions have made it harder for physicians to prescribe opioids. Gabapentinoids: What Are They?
As a result of the negative publicity and constraints about opioids, many people who are in severe pain have been left without relief. Consequently, physicians are searching for other drugs they can prescribe instead of narcotics. They may turn to gabapentinoids (gabapentin and pregabalin).
Gabapentin (Neurontin) and pregabalin (Lyrica) are both used to treat nerve pain. Doctors prescribed these medications three times more often in 2015 than they did in 2002, despite no radical change in the number of patients with neuropathic pain (JAMA Internal Medicine, online Jan. 2, 2018). The author advises his colleagues to use these drugs cautiously:
“The combination of a dearth of long-term safety data, small effect sizes, concern for increased risk of overdose in combination with opioid use, and high rates of off-label prescribing, which are associated with high rates of adverse effects, raises concern about the levels of gabapentinoid use. While individual clinical scenarios can be challenging, caution should be advised in the use of gabapentinoids, particularly for those individuals who are longterm opioid users, given the lack of proven long-term efficacy and the known and unknown risks of gabapentinoid use.”
A perspective published in the New England Journal of Medicine goes even further (Aug. 3, 2017).
The authors note that guidelines from the CDC recommend acetaminophen and NSAIDs as first-line options for osteoarthritis and low back pain. The physicians point out that “acetaminophen is often ineffective, and NSAIDs are associated with adverse effects that limit their use…” They go on to say:
“The CDC guidelines also recommend gabapentinoids (gabapentin or pregabalin) as first-line agents for neuropathic pain. We believe, however, that gabapentinoids are being prescribed excessively — partly in response to the opioid epidemic”
They conclude:
“Patients who are in pain deserve empathy, understanding, time, and attention. We believe some of them may benefit from a therapeutic trial of gabapentin or pregabalin for off-label indications, and we support robust efforts to limit opioid prescribing. Nevertheless, clinicians shouldn’t assume that gabapentinoids are an effective approach for most pain syndromes or a routinely appropriate substitute for opioids.”
Gabapentin Side Effects: The history of gabapentin (Neurontin) is fascinating. It was originally approved by the FDA for treating epilepsy in 1993. There is a tale of woe and intrigue about how the company that marketed Neurontin got into trouble with the FDA for illegal off-label marketing practices. We won’t go into that here, but you can read all about it in this article: Surprising Gabapentin Side Effects Gabapentin has become a go-to drug for doctors who are trying to control chronic pain problems. At last count, dispensed prescriptions have gone from 39 million in 2012 to 51 million in 2014 to 64 million in 2016 (Quintiles IMS, May 2017, now IQVIA Institute).
Gabapentin can cause depression, dizziness, fatigue, drowsiness, digestive tract upset, trouble with balance, cognitive difficulties, and visual problems. The official prescribing information warns:
“Antiepileptic drugs (AEDs), including gabapentin, increase the risk of suicidal thoughts or behavior in patients taking these drugs for any indication. Patients treated with any AED for any indication should be monitored for the emergence or worsening of depression, suicidal thoughts or behavior, and/or any unusual changes in mood or behavior.”
In 2014, a survey of more than 1,300 fibromyalgia patients by the National Pain Foundation and National Pain Report found medical marijuana is more effective than Lyrica, Cymbalta, or Savella, the three drugs approved by the Food and Drug Administration to treat the disorder. (If you’re curious about the effectiveness of Lyrica, Cymbalta, and Savella, then you might be interested in my post, “Why your fibro meds aren’t working.”)
There’s growing anecdotal evidence that marijuana relieves fibromyalgia pain, but actual research is still scant. Cannabis remains a Schedule I controlled substance in the United States, making it difficult for researchers to study the plant’s pain-relieving properties. To date, there have been less than a handful of small studies using cannabis or its derivatives to treat fibromyalgia. Most of those have shown it to be beneficial, especially for pain relief.
But why does cannabis seem to work so well? Dr. Ethan Russo, medical director of PHYTECS, believes fibromyalgia’s multifaceted symptoms may be caused by a deficiency in the body’s endocannabinoid system (ECS), a condition he calls Clinical Endocannabinoid Deficiency (CED). Maybe the reason cannabis is so effective is that it’s simply supplementing what the body needs – similar to how people take a supplement to treat vitamin D or B12 deficiency.
Russo explores the evidence behind his hypothesis in a soon-to-be-published review entitled, “Clinical Endocannabinoid Deficiency Reconsidered: Current Research Supports the Theory in Migraine, Fibromyalgia, Irritable Bowel, and Other Treatment-Resistant Syndromes.” While his idea is still theoretical, there is some early research indicating he may be onto something.
The ECS is made up of cannabinoid receptors within the brain, spinal cord, nerves, gut, organs, and other locations in the body. It helps the body maintain homeostasis and is involved in a number of physiological processes, including pain sensation, mood, memory, and appetite, among others. The body naturally makes endocannabinoids – the same kinds of endocannabinoids found in cannabis – that feed the ECS and keep it functioning.
Fibromyalgia causes symptoms throughout the body, with the primary ones being a pain, fatigue, cognitive and sleep difficulties. Certain conditions, like irritable bowel syndrome (IBS) and migraine, are extremely common among those with fibromyalgia – so much so that Russo believes they may all be connected to an ECS deficiency.
His theory makes sense. The ECS plays a role in so many of the body’s major systems, so if it was indeed malfunctioning, that would account for why fibro sufferers have such varied symptoms. Supplementing the ECS with cannabinoids from the cannabis plant would, in theory, relieve symptoms because the deficiency is being treated.
Russo first posited that fibromyalgia, IBS, and migraine may be caused by an ECS deficiency back in 2001. (Click here to read his first review on the subject.) His latest review gives an update on new research that supports ECS deficiency as a possible culprit for fibromyalgia, IBS, and migraine.
“Additional studies have provided a firmer foundation for the theory,” he writes in the review, “while clinical data have also produced evidence for decreased pain, improved sleep, and other benefits to cannabinoid treatment and adjunctive lifestyle approaches affecting the endocannabinoid system.”
CED is based on the premise that many brain disorders have been linked to neurotransmitter deficiencies. For example, dopamine has been implicated in Parkinson’s disease, and serotonin and norepinephrine have been associated with depression.
“If endocannabinoid function were decreased, it follows that a lowered pain threshold would be operative, along with derangements of digestion, mood and sleep among the almost universal physiological systems sub-served by the ECS,” Russo writes.
That’s a mouthful, but essentially it means if the ECS isn’t properly working, then it could account for the pain, sleep, digestive and other issues so common among fibromyalgia patients. Adding cannabinoids to the body through the use of cannabis may help to bring the ECS back into balance.
“It’s a key in a lock in your body that exists for a reason,” explains Dr. Jahan Marcu, chief scientist with Americans for Safe Access. “We send in cannabinoids to activate this system that’s supposed to be working. It’s a sort of care and feeding of the ECS so it can do its job.”
The best evidence for CED comes from an Italian migraine study, which found reduced levels of an endocannabinoid known as anandamide in patients with chronic migraines versus healthy controls.
“Reduced [anandamide] levels in the cerebrospinal fluid of chronic migraine patients support the hypothesis of the failure of this endogenous cannabinoid system in chronic migraine,” read the study.
Unfortunately, the Italian study will probably never be repeated in the United States because it required risky and invasive lumbar punctures.
In the gut, the ECS modulates the movement of food along the digestive tract, the release of digestive juices to break down food, and inflammation.
Cannabis has long been used to treat digestive issues and was one of the first effective treatments for diarrhea caused by cholera in the 19th century.
“Unfortunately while many patient surveys have touted the benefit of cannabinoid treatment of IBS symptoms, and abundant anecdotal support is evident on the Internet, little actual clinical work has been accomplished,” Russo writes.
A few studies using marijuana for fibromyalgia have had positive results. Overall, marijuana has been found to decrease pain and anxiety, and improve sleep and general well-being.
“There is actually some evidence that the levels of at least one endocannabinoid (anandamide) increase in the circulation of patients with fibromyalgia,” says Prof. Roger G. Pertwee from the University of Aberdeen in Scotland. “There is also considerable evidence that anandamide is often released in a manner that reduces unwanted symptoms such as pain and spasticity in certain disorders. … It is generally accepted that THC, the main psychoactive constituent of cannabis, can relieve pain, including neuropathic pain for example, by directly activating cannabinoid receptors. … Some non-psychoactive constituents of cannabis have also been found to relieve signs of pain, at least in animal models.”
For anecdotal evidence, Russo cites the National Pain Foundation/National Pain Report survey in his review, saying, “The results of the survey strongly favor cannabis over the poorly effective prescription medicines. These results certainly support an urgent need for more definitive randomized controlled trials of a well-formulated and standardized cannabis-based medicine in fibromyalgia inasmuch as existing medicines with regulatory approval seem to fall quite short of the mark.”
More research needs to be done to either prove or disprove CED’s existence.
“What we really need is randomized controlled trials to look at this more carefully, and that’s the only kind of evidence that the [Food and Drug Administration] and most doctors are going to find acceptable in the end,” Russo says.
MRI and PET scans are not yet able to detect endocannabinoid levels in living patients, but as technology advances, that may become a possibility. The ability to actually test endocannabinoid levels in fibromyalgia patients and compare those against healthy controls would help to confirm Russo’s theory.
“We’re on the edge of having that capability,” Russo says. “It’s in my plans to look at this type of thing in the future.”