Fibromyalgia symptoms can mask the presence ofchronicinflammatory disease affecting the joints of the pelvis and spine, according to new research.
The study, titled “Prevalence of Axial Spondyloarthritis Among Patients With Fibromyalgia: A Magnetic Resonance Imaging Study With Application of the Assessment of SpondyloArthritis International Society Classification Criteria,” was published in the journal Arthritis Care & Research.It highlights the importance of vigilant management of fibromyalgia symptoms by doctors and patients, taking into account the possible underlying presence of inflammatory disorders.
Unlike other rheumatologic diseases, fibromyalgia is non-inflammatory in nature, and recent reports suggest that it is caused by uncontrolled hyper-activation of the pain-associated nervous response.
Fibromyalgia patients can present a broad spectrum of symptoms, including chronic nocturnal back pain, morning stiffness, and disturbed sleep. However, these are also symptoms of an inflammatory condition called axial spondyloarthritis (SpA).
The spA is a chronic inflammatory condition involving the spine, pelvis, and surrounding joints. Although SpA and fibromyalgia are very different diseases, they can overlap and share similar symptoms.
Aiming to determine the incidence of SpA among fibromyalgia patients, a total of 99 patients with fibromyalgia underwent magnetic resonance imaging (MRI) evaluation for the identification of structural alterations common in SpA chronic inflammation1, such as bone erosion and spine deformations (sclerosis).
About 8% of patients presented symptoms of inflammation in pelvic joints, while 17% and 25% presented bone erosion and sclerosis, respectively. Despite the frequency of these symptoms, only 10% of fibromyalgia patients were positively SpA diagnosed,accordingto the Assessment of SpondyloArthritis International Society classification criteria.
“When approaching the clinical conundrum of differentiating between ‘pure’ fibromyalgia and those cases with an unsuspected underlying inflammatory disease, the physician must attempt to rely[on] onclinical judgment and on available diagnostictools,” the study’s authors, from medical centers in Tel Aviv, Israel, wrote.
Through blood tests that evaluate levels of a protein associated with inflammation, known as CRP, the authors found that the diagnosis of SpA was positively associated with increased CRP levels and physical function limitation. This result suggests that CRP could be used as a diagnostic tool for SpA among fibromyalgia patients.
“These results underscore the importance of recognizing the overlap between inflammatory and centralized pain in each patient and call for increased clinical vigilance in the process of differential diagnosis,” the authors concluded.
According to a study titled “Lengthened Cutaneous Silent Period in Fibromyalgia Suggesting Central Sensitization as a Pathogenesis” and published in the journal PLOS One, dysfunction in spinal cord processing may be responsible for pain in fibromyalgia (FM) patients.
Among other side effects, Fibromyalgia is portrayed by chronic widespread pain, but the root cause that is responsible for chronic pain in FM is still vague. A recent study has shown that for fibromyalgia pathogenesis, central pain amplification is key, FM pathogenesis also known as “central sensitization” is a process that is characterized by augmented pain and sensory processing in the spinal cord and brain.
The cutaneous silent period (CSP), a spinal reflex interceded by A-delta cutaneous afferents that are used to evaluate pain processing in both the central and peripheral nervous systems, between FM patients and normal healthy controls were compared by the researchers. The amount of people that were analyzed was 24 fibromyalgia patients (diagnosed according the 1990 American College of Rheumatology classification system) and 24 healthy controls of same age and sex. CSP was checked from the abductor pollicis brevis muscle which is present in the hand between the wrist and the base of the thumb by using standard electro diagnostic equipment, along with patients’ parameters in which statistic information, number of tender points, visual analog scale and fibromyalgia affects surveys scores were included.
These findings suggest that in the central nervous system, fibromyalgia is linked with pain modulation mechanisms dys-functioning. Also, according to researchers study, there was no correlation between CSP and clinical parameters like VAS score, K-FIQ score, age, and height, which postures questions in the matter of whether to utilize CSP to survey ailment seriousness. As a matter of fact, researchers emphasize that extra reviews are required to additionally assess the relationship between CSP parameters and clinical information.
The authors write in their report, “In conclusion, dysfunction of supraspinal control may be responsible for pain in FM, giving additional proof that central sensitization underlies the pathogenesis of the disease,”
Did you have a gynecologic surgery, such as a hysterectomy, in the few years before you developed fibromyalgia?
It’s a trend some people have noticed, and a study published in 2015 shores up the link between these types of surgeries and fibromyalgia onset. It also provides further evidence for an association between fibromyalgia and common overlapping conditions that are gynecologic, endocrine, or autoimmune.
Findings
In the study, researchers reviewed charts of 219 women with fibromyalgia and 116 women with non-fibromyalgia chronic pain. Specifically, they examined the time between illness onset and gynecologic surgery as well as the number of overlapping conditions in each group.
They also found that each of the three diagnosis types they were looking at was independently associated with fibromyalgia. Thyroid disease and gynecologic surgery were significantly more common in women with fibromyalgia than those with other types of chronic pain.
The timing of the gynecologic surgeries in relation to pain onset was especially interesting. They found more surgeries in the years just before fibromyalgia pain began, or in the year after pain onset. That pattern was unique to the fibromyalgia group.
At first glance, it may seem odd that gynecologic surgeries in the year after pain onset would be considered related to the development of fibromyalgia.
However, an association like that may be due to several pertinent factors.
For example, consider that many women have gynecologic problems well before they opt for surgery as the preferred treatment. It may be that hormonal changes or gynecologic disease are risk factors for fibromyalgia because of some underlying relationship that we don’t yet understand.
According to the study, hysterectomies and oophorectomies (removal of the ovaries) were most likely within the four years before or after the onset of fibromyalgia pain.
This is certainly an area that calls for more research. In the end, it could help us understand why 90 percent of fibromyalgia patients are women. Beyond that, it may reveal physiological changes that can trigger the development of the illness, which could lead to better treatments and possibly even prevention.
For the women who develop fibromyalgia after gynecologic surgery, we also need to know what role, if any, the surgery itself plays, as well as the possible roles of hormonal changes caused by the surgery. Post-surgical hormone replacement therapy deserves a look, too.
Doctors have long suspected that fibromyalgia has strong hormonal ties and triggers. A 2013 study found links between early menopause and increased pain sensitivity in fibromyalgia patients, which may relate to dropping estrogen levels.
Women with fibromyalgia are especially prone to painful menstrual periods (dysmenorrhea) and certain pregnancy complications.
My Experience
This study really speaks to my own experience. I was 34 when my youngest child was born via c-section, and 35 when I stopped breastfeeding. The hormonal changes from that, according to my gynecologist, launched me into premature perimenopause.
My menstrual cycle became erratic and periods were extremely heavy and painful, whereas they’d always been regular and fairly mild. Fibromyagia symptoms soon followed.
Six months later, I had a diagnosis and had identified a pattern—my flares came regularly between ovulation and the start of my period. My gynecologist recommended an endometrial ablation to get rid of hormones put off by the thickening uterus.
I hadn’t had a hysterectomy, but between two pregnancies and two c-sections, plus breastfeeding, my body had clearly been put through a hormonal ringer.
I suspect that research will continue to bear out the links between fibromyalgia and hormonal changes and hope that someday, we’ll be a lot better equipped to recognize, treat, and prevent hormone-related fibromyalgia.
Fibromyalgia has long baffled both medical professionals and sufferers. Branded as a neurological syndrome characterized by chronic pain, fatigue, and cognitive dysfunction, fibromyalgia has defied precise categorization and treatment. However, emerging evidence introduces a compelling and often-overlooked player in this painful puzzle: fascia, the connective tissue that blankets every inch of our internal architecture.
Could it be that the discomfort fibromyalgia patients endure—those deep, radiating aches and that crawling, prickling sensation beneath the skin known as formication—isn’t just rooted in the brain, but in this intricate web of tissue just beneath the surface?
Let’s peel back the layers—literally and figuratively—of the human body to expose how fascial dysfunction might underpin fibromyalgia, and what that revelation means for the future of symptom management and healing.
What Is Fascia? The Underappreciated Matrix of the Body
Fascia is a thin, fibrous, and remarkably dynamic connective tissue that envelops every muscle, bone, nerve fiber, and internal organ. This fibrous matrix performs far more than structural duties; it is rich in sensory nerve endings and plays a critical role in proprioception, pain signaling, and internal communication.
Far from being inert packing material, fascia is alive with cellular activity and fluid dynamics. It:
Supports and stabilizes musculature and joints
Separates and connects anatomical structures simultaneously
Conducts mechanical signals, such as pressure and vibration
Interacts intimately with the central nervous system via embedded receptors
In essence, fascia is the body’s broadband network—and when that network becomes gnarled, compressed, or dehydrated, the resulting dysfunction can cascade throughout the system.
Fibromyalgia has traditionally been attributed to central sensitization—a condition in which the brain and spinal cord amplify pain signals. While this remains a crucial piece of the puzzle, it does not fully explain why the pain begins in specific areas, or why it’s often symmetrical, migratory, and resistant to common painkillers.
When this tissue becomes stiff, bound, or inflamed, it exerts abnormal pressure on nerves, impairs blood flow, and generates localized inflammation—all of which can mimic and potentially cause the widespread discomfort seen in fibromyalgia.
Formication is a tactile hallucination—a feeling that something is crawling on or under the skin. It often coexists with fibromyalgia and is profoundly distressing. While frequently linked to neuropathy or drug withdrawal, many fibro patients experience it without external triggers, suggesting a deeper somatic origin.
So how could fascia be responsible for this bizarre, bug-like sensation?
Entrapped Nerves: Fascial adhesions can compress sensory nerves, causing misfires that the brain interprets as crawling or tingling.
Abnormal Tension: Chronic fascial tightness distorts mechanoreceptor input, leading to bizarre tactile sensations.
Inflammatory Signaling: Fascia, rich in immune activity, may spark cytokine activity that sensitizes nerve endings.
Disrupted Fluid Flow: Impaired lymphatic and interstitial fluid movement due to fascial rigidity may alter skin sensation.
Together, these factors provide a plausible basis for formication as a peripheral-origin hallucination, originating in fascia and misinterpreted by the brain.
Recent studies show that fascia has a higher density of nociceptors (pain receptors) than muscle tissue. This suggests that pain attributed to “muscle soreness” may in fact originate in the fascia.
Imaging Insights
Ultrasound and MRI technologies have demonstrated that fibromyalgia patients often have thicker, less elastic fascia, especially in the trapezius, lumbar region, and lower extremities.
Cellular Inflammation
Biopsies and lab studies suggest that inflammatory markers in fascial tissues are elevated in fibro patients—supporting the theory of an immune-mediated fascial syndrome.
Feedback Loops Between Fascia and the Central Nervous System
Fascia doesn’t operate in isolation. It is intimately tied to the nervous system through:
Proprioceptors (sensors for movement and tension)
Baroreceptors (sensors for pressure)
Chemoreceptors (sensors for chemical signals like inflammation)
A stiffened or inflamed fascial environment sends constant “danger” signals to the brain, keeping the nervous system in a perpetual state of alert. This feeds into central sensitization, reinforcing both pain perception and emotional distress—a loop that’s tough to break without addressing the tissue dysfunction.
Many fibromyalgia patients have undergone a carousel of medications—from antidepressants to anticonvulsants to opioids—without sustainable relief. Addressing the mechanical and physiological health of fascia offers a promising avenue.
Integrative Care Model
An ideal fibromyalgia treatment plan might include:
There’s growing recognition that the nervous system does not operate in a vacuum. It is embedded within the fascia, nourished by its fluids, and influenced by its tension. When fascia falters, nerves suffer—and the body broadcasts its distress through pain, fatigue, cognitive fog, and bizarre sensations like formication.
By embracing fascia as a living, reactive, and treatable structure, we open new doors for people with fibromyalgia—doors that may lead to recovery, restoration, and resilience.
Remember:
Formication and fibromyalgia share common neural roots—an interwoven story of sensory misfiring. Though unwelcome and at times terrifying, this symptom responds to a multi-pronged plan grounded in nerve modulation, holistic care, medical oversight, and patient resilience. By embracing a broad, informed approach, individuals suffering from formication can reclaim comfort, control, and, above all, hope.
More Detail about Formication and Fibromyalgia: When It Feels Like Bugs Crawl Beneath Your Skin
Fibromyalgia is a multifaceted disorder. Beyond chronic musculoskeletal pain and profound fatigue, sufferers often report a constellation of distressing sensory symptoms. Among them, formication—the eerie sensation of insects crawling on or under the skin—emerges as one of the most unnerving. Its existence in fibromyalgia raises questions about the nature of the disease: Why would a person feel tiny creatures writhing beneath the surface? Why is it so common among fibromyalgia patients? And how can one manage or treat such a disturbing sensation?
Formication (pronounced for-MIH-kay-shun) is the clinical term for the illusion or hallucination of insects crawling on or under the skin. Derived from the Latin formica (“ant”), it classifies as a tactile hallucination—a sensory misperception where the skin feels touch, pressure, or movement that has no external source.
Psychosomatic or Neurological?
Although formication frequently appears in psychiatric conditions and stimulant drug use, such as chronic methamphetamine abuse, it is not solely a mental health phenomenon. The culprit is a misfiring nervous system—sensory signals being generated without any actual stimulus. The brain interprets these signals as crawling sensations, triggering a powerful, visceral reaction, even though no real bugs are present.
Why It’s So Distressing
Psychological torment: The sensation can feel all too real—driving sufferers to itch, scratch, or pick compulsively.
Docked sleep: The relentless crawling feeling can interrupt rest, triggering further physical and emotional exhaustion.
Risk of self-inflicted harm: Constant scratching may lead to open sores, infections, scarring, and a vicious cycle of pain.
Emotional strain: The awareness that others may not believe you only adds to isolation, frustration, and uncertainty.
Fibromyalgia is increasingly understood as a central nervous system disorder, in which pain and sensory signals are amplified or misinterpreted. Just as fibromyalgia patients experience widespread pain and hyperalgesia (heightened sensitivity to painful stimuli), they may also experience tactile misinterpretations like formication.
Consider these points:
Altered pain thresholds: In fibromyalgia, pain signals can arise spontaneously; likewise, sensations like crawling may emerge without an external cause.
Crosstalk in sensory pathways: Overlapping neural circuits for pain and touch might misfire, confusing tactile signals.
Central sensitization: The brain becomes primed to detect threats, turning up the volume on stimuli—real or imagined.
Data Supporting the Connection
Many fibromyalgia patients report complex sensory symptoms:
Itching without skin changes
Burning or tingling sensations (paresthesia)
Peripheral swelling, unexplained by visible inflammation
Though medical research into formication in fibromyalgia is still developing, existing studies point to its high prevalence and strong association with other sensory disturbances—reinforcing the theory of shared neural dysfunction.
Lack of large-scale studies on its prevalence and pathophysiology
Limited neuroimaging evidence to pinpoint brain regions responsible
No clear “standard of care”, leading patients to navigate trial-and-error treatments
Variability among individuals—what alleviates symptoms in one person may be useless for another
9. Emerging Research & Future Directions
The scientific community is steadily advancing understanding:
Neuroimaging studies are mapping abnormal sensory processing in fibromyalgia—hinting at targets for neuromodulation.
Peripheral neuropathy investigations reveal micro-nerve damage in many fibro patients, which may trigger formication.
Novel therapeutics, including low-dose naltrexone, cannabinoids, IVIG, and even brain stimulation (TMS, tDCS), are under scrutiny for their nervous-system modulating effects.
10. Empowering Yourself: Tips & Takeaways
Understand it’s real—Formication is not imaginary or psychological weakness.
Reduce self-harm—Trim nails, use moisturizers, and apply chill compresses.
Track episodes—A diary reveals triggers and aids medical planning.
Treat the nerves—Address fibromyalgia itself, not just individual symptoms.
Harness mind-body tools—Meditation, CBT, and relaxation techniques help regulate neural signals.
Advocate for care—Work with clinicians toward multidisciplinary treatment.
Stay hopeful—Research progresses, and many fibromyalgia patients find relief with personalized strategies.
11. Stories from the Front Lines
To grasp the lived reality of formication, consider these patient-reported experiences (anonymized):
“It felt like ants were marching all over my arms. I’d wake up in the middle of the night scratching until I bled. Nothing calmed it—no coconut oil, no antihistamine. Finally, gabapentin helped me get through the night.”
“Doctors called me paranoid, but I knew I wasn’t going crazy. Writing in my journal, I realized every episode followed heavy coffee or my PMS week.”
Sleep hygiene, relaxation routines, possible sleep meds
Skin Damage
Scratching leads to wounds and potential infection
Nail care, soothing compresses, monitor lesions, treat promptly
Emotional Distress
Anxiety, helplessness, fear of being misunderstood
Support groups, clear communication, stress reduction tactics
Doctor-Patient Misalignment
Central nature complicates understanding
Education, documentation, advocate for neuro/derm care and biopsies if necessary
13. Final Thoughts: You Are Not Alone
Dealing with fibromyalgia is already a full-time struggle—juggling pain, fatigue, “fibro-fog,” and emotional ups and downs. To add formication—sensations of ants, worms, or bugs crawling on your skin—often unmasks profound frustration. But the sensation is not random or imagined—it is a symptom of nervous system chaos, not a character flaw.
By acknowledging its connection to fibromyalgia, documenting episodes, advocating for nerve-directed treatments, and adopting skin-friendly and mind-body measures, you can gain control, reduce episodes, and protect your well-being.
Further Resources & Reading
Fibromyalgia research foundations—offer patient-oriented guidance and clinical trial listings
Neurosensory and neuroimaging journals—for emerging insight into tactile hallucinations and central sensitization
Support communities—both local and online—for shared strategies, empathy, and hope
Final Reflections: Rewiring the Body Through Tissue Healing
Fascia may not be visible to the naked eye, but it speaks volumes through the language of sensation. In fibromyalgia, its voice is often muffled—drowned out by pain pills and misunderstood diagnoses. But when we listen closely, fascia may hold the key to unraveling the chronic pain that shadows so many lives.
No single therapy will be a silver bullet. Yet, through patient-centered, fascia-inclusive care, fibromyalgia sufferers can begin to stitch together a tapestry of healing—one strand of relief at a time.
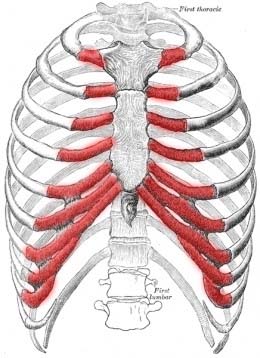
Many fibro patients suffer from a condition called Costochondritis, apart from common symptoms of fibromyalgia. In this condition, wearing a bra becomes difficult and sometimes even becomes impossible because it causes pain in the rib cage and breasts. Wearing the right bra can reduce the pain significantly if you are suffering from Costochondritis.
Inflammation of the cartilage that links the ribs to the breast bone is Costochondritis. It is very sudden and causes immense chest pain, much of fibromyalgia pain begins with this pain. Is the pain mildly irritating or it is extremely irritating, this all depends on the amount of inflammation, patients suffer from. Some patients describe what they go through as burning, stabbing, or aching pain. Some patients suffer from a complex chain of pain that they even relate to a heart attack.
In this condition, it is a painful task to put on tight clothing which compresses the ribs and needless to say an underwear bra. To reduce the pain wearing a comfortable bra is necessary to get rid of breast and ribcage inflammation but many women do not do this. However, when needed, it is best to wear something not too tight, in a comfortable fabric, and easy to wear and remove. Here are some tips for the selection of the right bra:
Seamless bra types are ideal as they prevent edgings from pressing against the skin.
Prevent that type of fiber that brushes against the skin and causes pain by avoiding anything textured like lace, tulle, or fabric with embroidery.
Best bra styles for every size
Soft cup bras: these bras offer good support for women of all sizes. Choose something with wilder shoulder straps as they won’t dig into the skin like the thinner ones do. A front closure design would also reduce the pain of putting on and removing the bra.
Sports bras: these bras can be very easy and comfortable as they give support to women of all sizes. Opt for something softer and with a wider stretch to prevent squeezing your ribcage and causing pain.
Bralettes: for smaller-sized women, a bralette might work in a good way. They are usually made with soft cups and are mildly comfortable.
Bandeaus: it is another good option for small and medium-sized women because bandeaus will sure that no wires or edges would press against the skin.
Dysphagia is a medical term that means that a patient has difficulty swallowing. There are a number of different conditions that can cause dysphagia. And someone who suffers from dysphagia often finds that it makes life very difficult. Depending on their condition, swallowing can be very painful, which makes eating and getting enough nutrition a challenge.
And what’s even more alarming is that many people with fibromyalgia report having problems with dysphagia.
So, what are some of the things that can cause dysphagia? Is there a link between the condition and fibromyalgia? And what can you do to treat it?
There are a number of different things that can cause dysphagia. Anything that interferes with the complex system of nerves and muscles that control the esophagus can make swallowing difficult. But some of the most common causes are:
Achalasia– a condition that causes the muscles in the esophagus to constrict.
Diffuse Spasm– a condition where the muscles spasm uncontrollably, usually after swallowing.
Esophageal Stricture– a narrowing of the opening of the esophagus caused by scar tissue or tumors.
Gastro-Intestinal Reflux Disease (GERD)– The gradual destruction of the tissue in the esophagus caused by acid from the stomach washing up into the esophagus.
Dysphagia can also occur without any obvious source. But whatever the cause, the symptoms are often similar. The most common symptoms are difficulty swallowing, pain in the throat, frequent heartburn, a hoarse voice, and regurgitating food you’ve already eaten.
In most cases, dysphagia isn’t dangerous. But it can lead to dramatic weight loss and can be life-threatening if it causes you to regurgitate food into the lungs.
And while we don’t always know what causes the condition, we do know that it is abnormally common in people with fibromyalgia.
A study by the National Institute of Health in the United States determined that a significant number of patients with fibromyalgia reported problems with swallowing. Patients in the study reported suffering from dysphagia at a rate 40% higher than people without fibromyalgia.
Unfortunately, the reason this sort of symptom is common in people with fibromyalgia remains a mystery. There’s so much that we don’t know about how fibromyalgia works, including why it would cause dysphagia. But we can speculate on a number of possibilities.
People with fibromyalgia often experience muscle weakness. This weakness could explain why they suffer from dysphagia. The muscles that control the process of swallowing may be affected by the general weakness caused by fibromyalgia.
In addition, we know that people with fibromyalgia have problems with their nervous system. An NIH study found that patients with fibro had significantly more neurological abnormalities than a control group. If fibromyalgia is a condition that affects the nervous system, as many doctors suggest it is, then it could be causing a breakdown between the nerves that control the esophagus and the brain.
This would explain why people with fibromyalgia have a hard time swallowing. Their brain can’t control the muscles in the esophagus as they normally would. But until we know more about the condition, we can’t say for sure what the link is. Luckily, there are some things you can do to treat the condition.
The first step in treatment is a diagnosis. The most common way to diagnose the condition is with an imaging test, like a barium X-ray. Essentially, the patient drinks a contrast material – barium- which coats the esophagus and makes it easier to see on the X-ray. The doctor can then examine the image to see if your esophagus is expanding correctly. And this examination can also be done with an endoscopic camera.
Your treatment will depend on what’s causing the condition. If the condition is caused by weakened muscles, there are a number of exercises you can do to strengthen the muscles. And you can learn different swallowing techniques to compensate for the weakened muscles. Your doctor will be able to advise you on what to do.
If the treatment is caused by muscle constriction in the esophagus, there are a number of medications that can help relax the muscles. In addition, a surgeon can perform a procedure to dilate the muscles and force them to relax. Finally, a surgeon can remove portions of the esophagus to widen the space for food to pass through.
If you’re experiencing difficulties swallowing, it’s always a good idea to see a doctor. They will be able to give you advice on the best course of treatment.
Many fibromyalgia sufferers have been told that the pain is “all in their head.” New research indicates there may be some truth to that, and that overactive brain networks could play a role in the hypersensitivity of fibromyalgia patients.
Fibromyalgia is a poorly understood disorder characterized by deep tissue pain, fatigue, headaches, mood swings, and insomnia. There is no known cause and successful treatments have been elusive.
In a lengthy study published in the journal Scientific Reports, an international team of researchers at the University of Michigan and in South Korea report that patients with fibromyalgia have brain networks primed for rapid responses to minor changes. This abnormal hypersensitivity is known as called explosive synchronization (ES).
“For the first time, this research shows that the hypersensitivity experienced by chronic pain patients may result from hypersensitive brain networks,” says co-senior author Richard Harris, Ph.D., an associate professor of anesthesiology at Michigan Medicine’s Chronic Pain and Fatigue Research Center.
In ES, a small stimulus can lead to a dramatic synchronized reaction throughout the network, as can happen when a power outage triggers a major grid failure or blackout. Until recently, this phenomenon was studied in physics rather than medicine. Researchers say it’s a promising avenue to explore in the quest to determine how a person develops fibromyalgia.
“As opposed to the normal process of gradually linking up different centers in the brain after a stimulus, chronic pain patients have conditions that predispose them to link up in an abrupt, explosive manner,” says first author UnCheol Lee, PhD., a physicist and assistant professor of anesthesiology at Michigan Medicine.
The researchers tested their theory by conducting electroencephalogram (EEG) tests on the brains of 10 female patients with fibromyalgia. Baseline EEG results showed the patients had hypersensitive brain networks, and that there was a strong correlation between the degree of ES conditions and the self-reported intensity of their pain during EEG testing.
Lee’s research team and collaborators in South Korea then used computer models of brain activity to compare the stimulus responses of the fibromyalgia patients to those of healthy ones. As expected, the fibromyalgia model was more sensitive to electrical stimulation.
“We again see the chronic pain brain is electrically unstable and sensitive,” Harris says.
Harris says this type of modeling could help guide future treatments for fibromyalgia. Since ES can be modeled outside of the brain in computers, researchers can test for influential regions that transform a hypersensitive network into a more stable one. These regions could then be targeted in living humans using noninvasive brain modulation therapies such as transcranial magnetic stimulation, which is currently used to treat fibromyalgia and depression.
“We expect that our study may ultimately suggest new approaches for analgesic treatments. ES provides a theoretical framework and quantitative approach to test interventions that shift a hypersensitive brain network to a more normal brain network,” researchers reported.
“It may be possible to convert an ES network to a non-ES network just by modulating one or two hub nodes. Indeed, transcranial magnetic stimulation and/or transcranial direct current stimulation may be improved by ‘targeting’ these sensitive hub nodes. The application of deep brain stimulation to critical nodes that could modify ES conditions is another therapeutic possibility that could be explored.”
Are the eyes the window to whatever’s going wrong with the brain in fibromyalgia? Research published in 2015 and 2016 suggests that it just might be.
Fibromyalgia is widely believed to be a condition of the central nervous system, which includes the brain and spinal column. It also includes the eyes and the structures that help our brains interpret what we see.
Chief among these structures is the optic nerve, which is similar to a cable made up of many smaller fibers.
Among them is a layer of nerves called the retina nerve fiber layer (RNFL).
Those nerve fibers are of special interest to researchers because of other recent work that’s uncovered dysfunction of the small nerve fibers. It suggests that, in people with fibromyalgia, small-fiber neuropathy (nerve damage) may be responsible for at least some of the pain.
In two studies, Spanish researchers have also discovered evidence of neuropathy in the small fibers of the eye.
In the study published in 2015, researchers looked at blood flow to the optic nerve and the RNFL. Blood flow, also called perfusion, is hypothesized to be irregular in several regions of the brains of people with fibromyalgia.
Researchers examined and took photographs of the eyes of 118 people with this condition plus 76 healthy people in the control group.
The photos were then analyzed with special software. The researchers concluded that the fibromyalgia eyes did in fact show low perfusion rates in several sectors, but the only significant difference was in certain RNFL.
The study published in 2016 built on that research, involving many of the same researchers. This time, they included 116 people with fibromyalgia and 144 in the control group.
They found:
a significant decrease in the RNFL in fibromyalgia compared to controls
a thinning of multiple structures in the eye
greater optic nerve thinning in those with severe fibromyalgia than in those with a milder case
greater optic nerve thinning in subgroups without depression than in those with depression
Before now, fibromyalgia has been considered non-neurodegenerative, meaning that no biological structures were being damaged or destroyed as they’re known to be in other neurological diseases such as multiple sclerosis or Alzheimer’s disease.
However, this research suggests that fibromyalgia may, in fact, involve some neurodegeneration in structures inside the central nervous system.
This, combined with earlier research on small nerve fiber damage in the skin, could mean that the degeneration is not confined to the central nervous system but may extend to the peripheral nervous system, which includes the nerves in the limbs, hands, and feet.
Fibromyalgia has always posed problems for doctors. We have pain, but no obvious cause. If this research is accurate, which we won’t know until it’s been replicated, it could mean that our pain comes from a very understandable source. After all, neuropathic pain has been recognized for a long time.
Suddenly, it makes our “mysterious” pain not mysterious at all.
On the other hand, it opens new doors for questioning. If we have damaged nerves, then why? What is causing the damage?
Possible candidates could include autoimmunity, which would involve the immune system going haywire and attacking the nerves as if they were bacteria or viruses, and problems with how the body uses substances that grow or maintain nerves.
Researchers have long speculated about possible autoimmunity in fibromyalgia, but so far we don’t have solid evidence pointing toward it. Now that researchers have discovered actual damage, they may gain better insight into where to look for autoimmune activity.
They may also be able to pinpoint shortages or inefficiencies in how nerves are maintained.
When it comes to diagnostic tests, it’s too early to say whether abnormalities in the eye could lead to a more objective test than we currently have. If so, it would be a major advancement in how fibromyalgia is detected.
Because the thinning was worse in more severe cases, it could provide a marker for doctors to monitor treatments as well as progression.
It’s also possible that these discoveries could lead to targeted treatments.
We won’t know the full impact of this research for some time, as any advancement in diagnostics and treatments would have to come after further research either confirms or contradicts these findings.
I’m a fairly open person when it comes to physical and mental illness, but I can also be very reserved, especially about my chronic pain and fatigue. It’s not because I don’t want to share about what’s going on with me, but because I don’t want people to think I’m a “whiner” or “attention seeker.” I am neither of those things. In fact, I’m quite the opposite.
A lot of people know I have fibromyalgia. What they don’t know is the reality of what I deal with. They see a positive, silly, young 25-year-old woman on the outside, but they don’t realize how much pain I’m in, or how badly my anxiety is affecting me. I don’t think people really understand the intensity of my conditions. I’ll admit that part of it is my fault, for showing only the good parts of my life on social media, but showing the not-so-good parts can sometimes come off as attention seeking. I don’t want attention, I want my conditions to stop being stigmatized. I don’t want pity, I want people to understand these illnesses.
When you tell someone you’re in pain, they don’t really take it very seriously. They usually think that you have a typical headache or backache. They don’t realize that your whole body is experiencing aches, stabbing pain, needles, numbness, or oftentimes a burning sensation. They also don’t realize that the clothing you’re wearing, or the cloth chair you’re sitting on could be causing you pain as well. People with fibromyalgia have sensitives to certain fabrics and materials. Some of us (including myself) feel pain in our organs. I’ve had ovarian pain for years and didn’t know what it was until I was diagnosed with fibromyalgia.
Our pain is often unbearable and can cause difficulties in everyday situations. When I’m going through bad flare-ups, I am sometimes late to work. It seems like no matter how early I wake up, it takes me 30 minutes to an hour to get out of bed because my body is stiff, my hips are locked, and my hands ache. Carrying a grocery basket can cause my hands and elbows to tense up, opening jars is sometimes impossible, household chores can take everything out of you, and the list could go on.
Speaking of being late to work, fatigue is another reason it’s so difficult to get out of bed. I could have had the best sleep of my life, but it will feel like I didn’t sleep a wink. For me, chronic fatigue is one of the most difficult symptoms. There have been days I’m nervous to drive long distances because the sun causes really bad fatigue. I work a desk job, but by midday, I feel like I’ve been doing hard labor, and all I want to do is go home and sit on the couch. And good luck trying to schedule anything with me after work. I’ll just be too exhausted to do anything. If you’re able to get me to hang out with you on weekdays, it’s probably because no matter how tired I am, I really need your company.
This is the last symptom I will touch on. Brain fog is a bitch, to say the least. Completely forgetting a conversation you had yesterday, having to pause mid-sentence because you forgot what you were saying, or stopping a conversation altogether because you can’t think of the right words to use. This is the most embarrassing symptom of fibromyalgia. Feeling incompetent is incredibly frustrating and heartbreaking. I often wonder if people are judging me because of this. I find at times, I can’t even remember how to spell a word when I’m typing. I proofread my text messages, emails, and social media posts multiple times before pressing the “send” or “submit” button. The embarrassment of brain fog causes me so much anxiety. I just want people to know can’t control the way my brain works sometimes.
It’s very common that individuals with fibromyalgia will struggle with different symptoms than others. All symptoms are different for everyone, so it’s difficult to explain to doctors what your symptoms are. Chronically ill patients seem to know about their illness than professionals, and that can be hard when it comes to medications and treatments. We’re all in this together, and we need support and understanding from the people and loved ones in our lives.
I hope this sheds some light on this awful illness. If you know someone living with fibromyalgia, go give them a (gentle) hug and ask what you can do to help them. Just being there to listen could mean the world!
Social Security has published a ruling that helps define when applicants with fibromyalgia should be granted disability benefits.
A lot of candidates for Social Security disability benefits the ones who apply based on fibromyalgia get rejected. The part of the motive was that Social Security does not have a disability “listing” for the condition. (Social Security’s disability listings offer the conditions needed for numerous different impairments to be sanctioned as disabilities.) The Social Security Administration (SSA) printed a ruling in 2012 to address the issue, providing directions to disability claims surveyors and administrative law judges (ALJs) regarding how to evaluate fibromyalgia circumstances. This ruling ought to help reduce the number of fibromyalgia applicants who are rejected at the preliminary application phase and go on to file an appeal and ultimately win disability welfares.
Despite that, a lot of fibromyalgia patients will continue to be denied welfares. If you are applying for disability constructed on fibromyalgia, it just benefits to know that how the SSA views this specific impairment (known as fibromyositis).
Usually, when a disability claims examiner got a situation where the motive for disability was just fibromyalgia, the point of view for an initial endorsement was poor. Disability examiners usually presented slight weight to an entitlement of fibromyalgia unless there was one more condition involved, for instance, degenerative disc disease or arthritis, the one that was more possible to come with objective proof of the disease just like x-rays. Why was it? Part of the problem has to do with the nature of fibromyalgia—its signs are mostly particular and its causes are not understood. Since its symptoms differ from person to person, and for the reason that the medical career had not figured out fibromyalgia’s reasons, disability examiners were by no means certain how to categorize such circumstances. As the medical profession has started to recognize fibromyalgia better, Social Security has established new standards for evaluating fibromyalgia.
As to be selected for disability welfares, you need to have an impairment recognized by medical proof for instance medical “signs” of the disease or illness and lab tests. In other words, your impairment cannot be established merely by your reports of your symptoms. This is known as the necessity of having a “medically determinable impairment” (MDI)—the SSA has to understand medical signs of an impairment that might more likely be expected to produce your symptoms. Verifying this can be challenging with fibromyalgia, as the illness is generally categorized by subjective reports of extensive pain, dizziness, tenderness in the muscles, joints, and soft tissues, fibro fog, and fatigue.
Luckily, in July 2012, Social Security allotted a ruling clarifying when fibromyalgia would bring into being as a medically determinable impairment. The ruling directs statements examiners and judges to count on conditions allotted by the American College of Rheumatology (ACR) to define whether a candidate has fibromyalgia, and so has an MDI.
To be considered an MDI first, the patient would have proof of chronic extensive pain, with pain in the back, chest, or neck and the doctor must have governed out other diseases (hypothyroidism, such as lupus, and multiple sclerosis) over the procedure of lab tests or x-rays. Also, the patient must have one of the following:
1. Tender arguments in at least 11 of 18 tender argument regions of the body, with tender arguments befalling on both sides of the body and both above and beneath the waist. You can get a list of the tender arguments in the SSA’s latest ruling on fibromyalgia.
2. Repetitive manifestations of six or additional fibromyalgia symptoms, mainly cognitive, fatigue, or memory issues (fibro fog), anxiety, non-restorative sleep, depression, or irritable bowel syndrome (IBS). Other likely symptoms consist of abdominal pain, headache, muscle weakness, seizures, Raynaud’s phenomenon, and dizziness.
The claims examiner will evaluate your medical records to see if they comprise proof of the above criteria. The examiner will read the doctor’s notes on your complaints of fatigue, pain, and possible cognitive complications. To evaluate the reliability of your complaints, the claims examiner can ask your doctor to offer information about the amount and time period of your impairments, his or her judgment of how well you are capable to function, what treatments were done, and whether they were supportive and had side effects, and how long the doctor believes your capability to function to be restricted. The longer your medical record contains proof of fibromyalgia symptoms and treatment, the better.
In case SSA defines that you have the medically determinable impairment of fibromyalgia, Social Security’s assessment is not done; actually, it has just started. The SSA will possibly create a “residual functional capacity” (RFC) assessment for you to decide if there is any work you can do, with your past work. RFC assessment is an estimation of your capability to perform numerous exertional stages of work; let’s say, if you can’t lift more than ten pounds, you will be provided a sedentary RFC. The SSA bases your RFC on your medical records, views from specialists and doctors, and statements from you and from your family members. In evaluating your RFC, the SSA will be dependent on your doctor’s view as to your abilities, just like how long you can stand, walk, and sit, how much you can lift, and how well you can focus and remember guidelines. These practical restrictions are the key to showing the SSA why you can’t work.
When making your RFC, the SSA will match it to the kinds of jobs vacant for somebody with your RFC level and restrictions. If the RFC rules out every job, though sedentary work, you will be considered disabled.
More likely in other cases, hiring a lawyer to request a rejection of welfares for fibromyalgia can surely benefit, as disability lawyers are aware of the Social Security decision on fibromyalgia (SSR 12-2p) and the modern court verdicts on when disability would be approved for fibromyalgia. This information can assist disability attorneys to find errors that were made by the judge or claims examiner in the disability determination and use them to your benefit.
Also, if just a primary care internist or physician gives you a fibromyalgia diagnosis, then try to make an appointment with a specialist; and a diagnosis made by a rheumatologist will be more reliable to a judge or disability examiner and will help your Social Security disability request or claim.